
If you have been scrolling through social media, you’ll find certain dermatologists commenting on the fallacy that retinoids can thin the skin. Most notably, Dr. Barbara Sturm claimed in a Wall Street Journal interview that she doesn’t recommend retinol/retinoids because they thin the skin.
Today, we’re going to dive deep into the science of how retinoids work and find out what could actually be driving this confusion amongst non-dermatologists.
The Science of Retinoids
As a researcher, I see in this statement a fundamental misunderstanding of how retinol and retinoids work, especially in terms of histological evidence surrounding decades worth of retinoid research. It’s also worthwhile to note that when it comes to the Asian skin phenotype—the topic is nuanced.
Effects on the Cellular Matrix
As a Korean study highlighted, East Asians possess a unique genetic susceptibility with regards to retinol/retinoid use. There are 30 genes identified linked to retinol intolerance.
We begin with this misconstrued idea that the skin is thinned by retinoids. We have to separate the epidermis from the dermis. When people say that retinoids thin the skin, they are likely referring to a temporary, superficial desquamation process.
- Retinoids accelerate desquamation.
- They cause the stratum corneum (the outermost layer of dead skin cells) to shed and become more compact.
- This gives the skin a glassy, translucent look, which can be misconstrued as the skin feeling thinner.
Retinoid Facies
In dermatology, we have an interesting term called retinoid facies, which describes the youthful, tight-looking complexion associated with years of retinoid use. This is actually associated with:
- Thickening of the dermis.
- Compaction of the stratum corneum.
While retinoids can cause transient barrier impairment and transepidermal water loss, they are a therapeutic staple in dermatology. Decades of in vivo biopsies and foundational research by Griffiths and colleagues prove that topical retinoids are helpful for:
- Stimulating Type I and Type III collagen synthesis.
- Increasing dermal thickness over a 12 to 24-week period.
- Rebuilding the skin’s structural foundation.
Retinoids don’t make your skin fragile; they make it structurally resilient.
Considerations for Sensitive Skin and East Asian Phenotypes
I must clarify that especially in skin of color and East Asian skin, retinoids can indeed cause increased skin irritation, by impairing the skin barrier and increased TEWL. But it is inaccurate to describe this as skin thinning.
Contraindications
The use of retinoids is likely a flat contraindication if you have:
- An already compromised skin barrier, such as eczema.
- A genetic deficiency in the gene for filaggrin (even without active symptoms, retinoids can unmask it).
The “Retinization” Phase
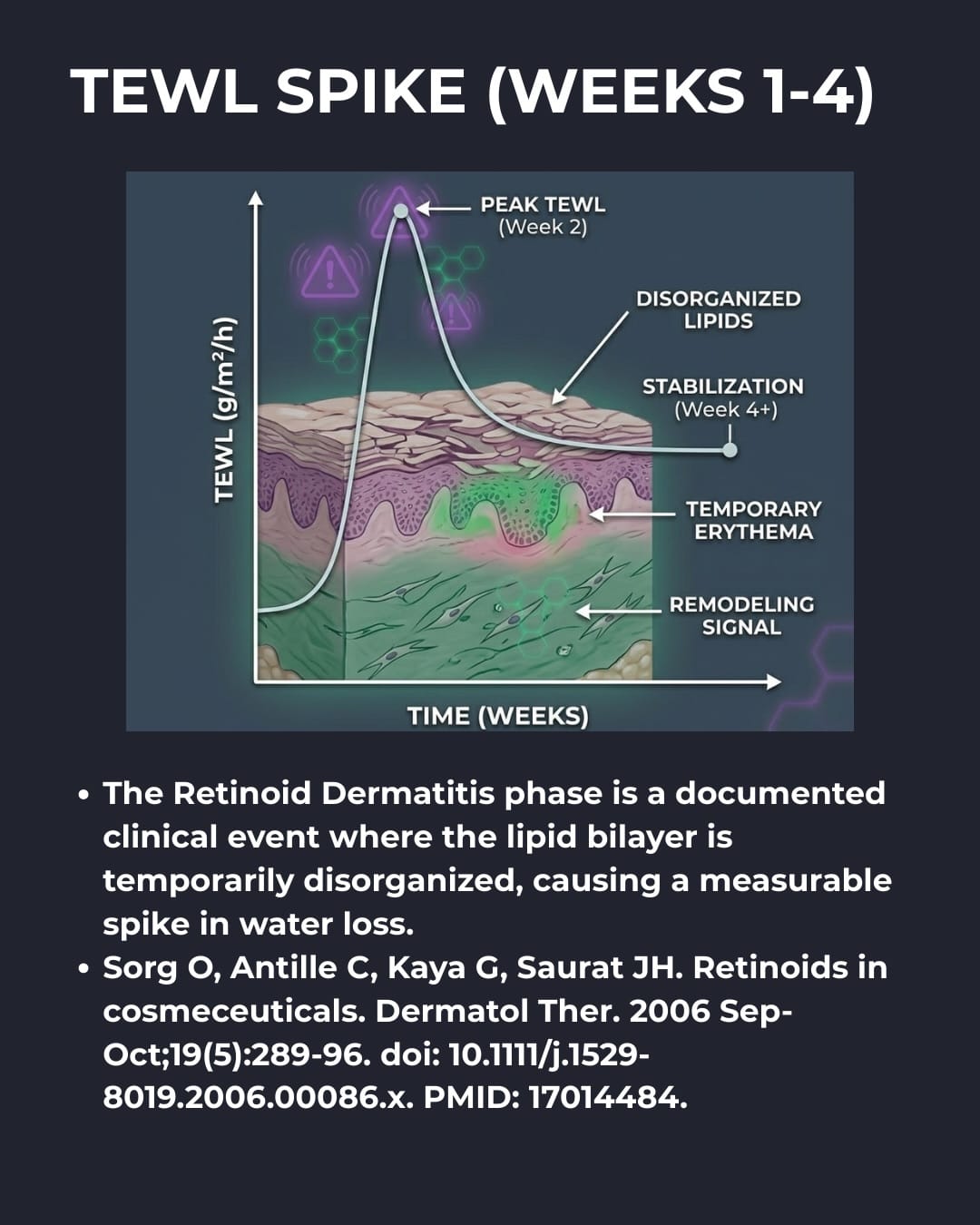
For healthy individuals, the first two to four weeks of use is the retinization phase. During this time:
- The retinoid penetrates and disrupts the lipid matrix.
- This causes a spike in transepidermal water loss.
While there is a positive benefit for most, as you grow older—or if you have dry skin, atopic dermatitis, or other conditions like perioral dermatitis or rosacea—you may lack the biological mechanism for adaptation. In these cases, retinoids can cause:
- Prolonged sensitization
- Chronic retinoid dermatitis
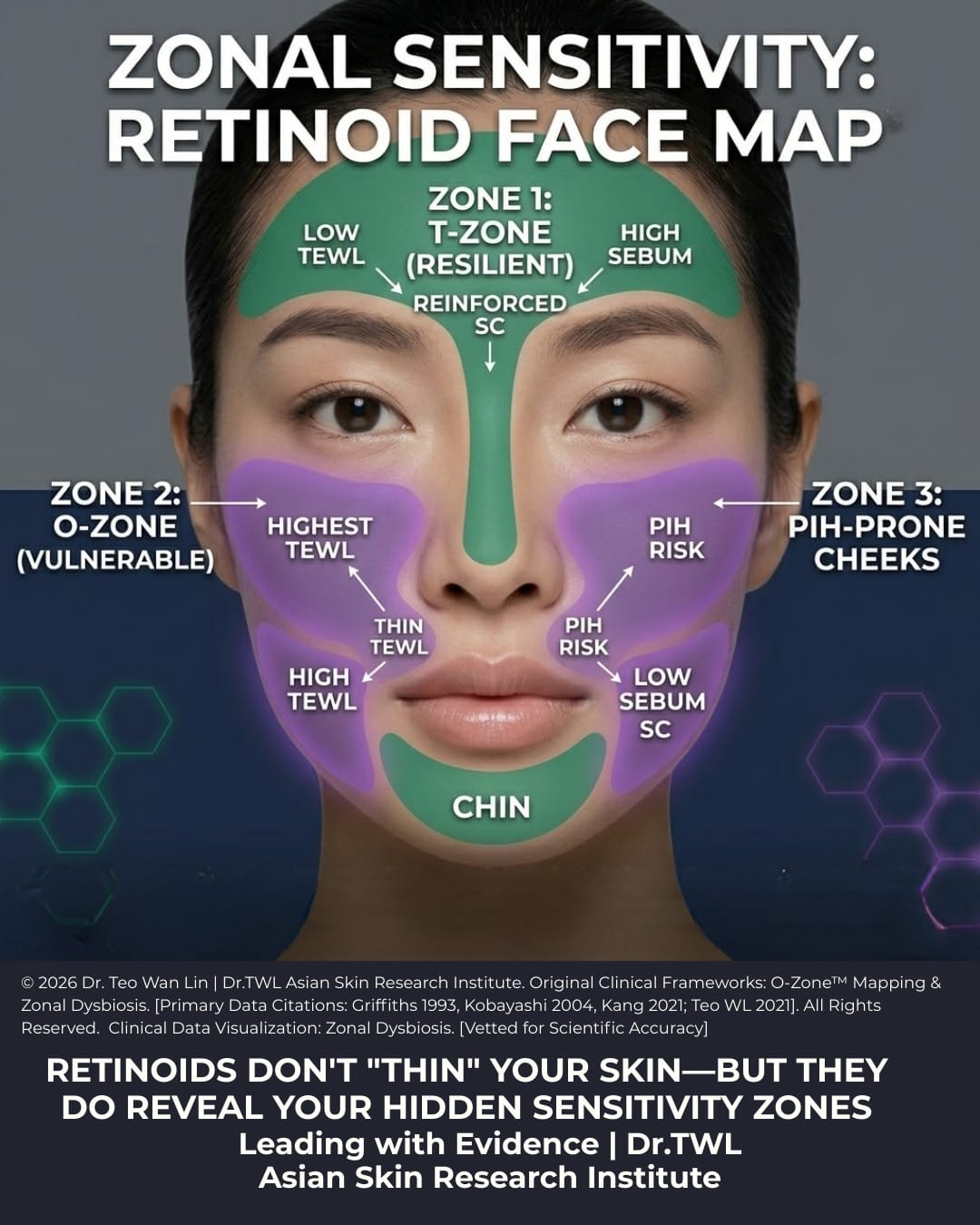
My Personal Experience in the light of facial zones
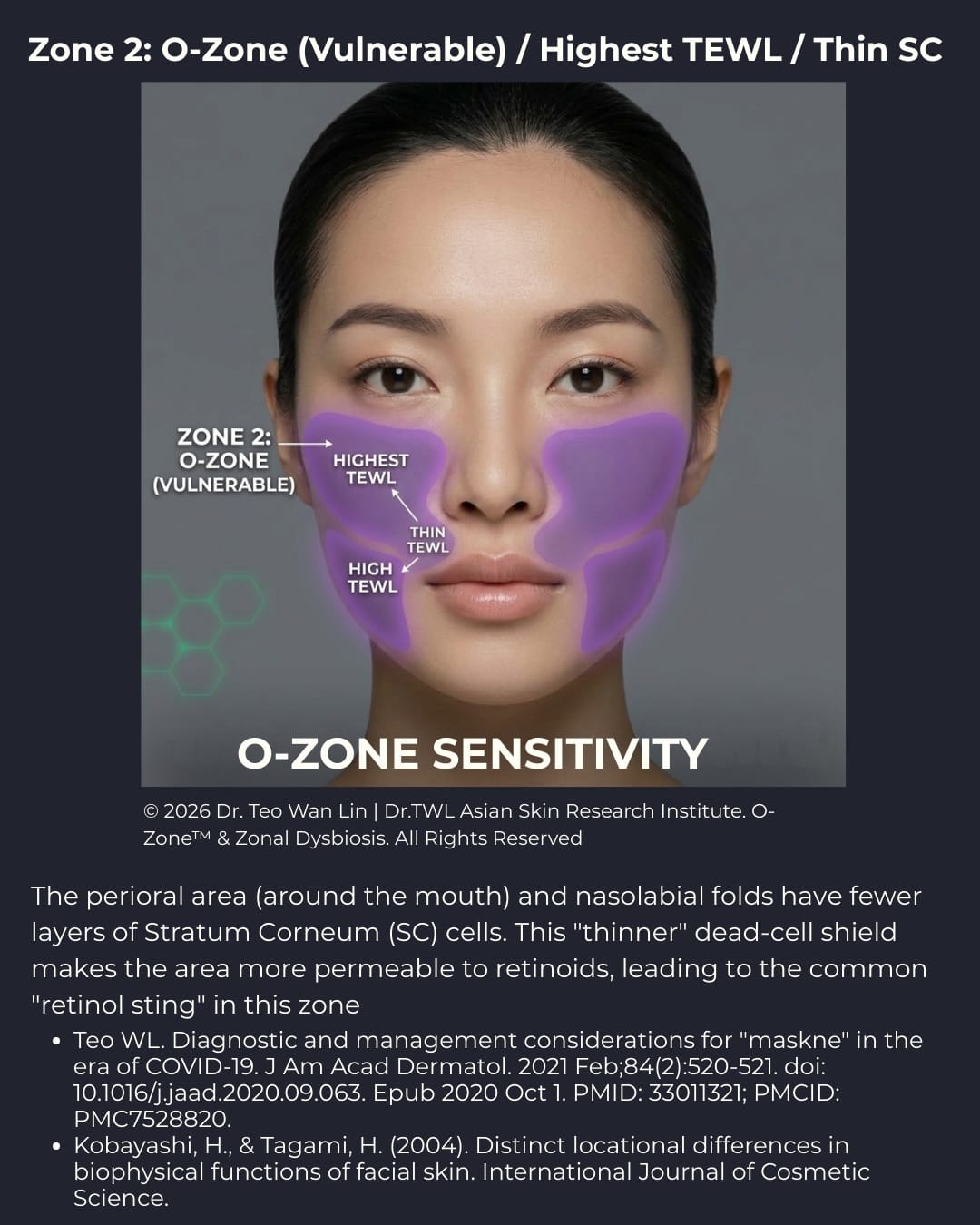
In my case, I tolerated retinoids well for almost two decades. When I hit my mid-30s, I developed sensitivity, most prominently in the perioral area and around the cheeks.
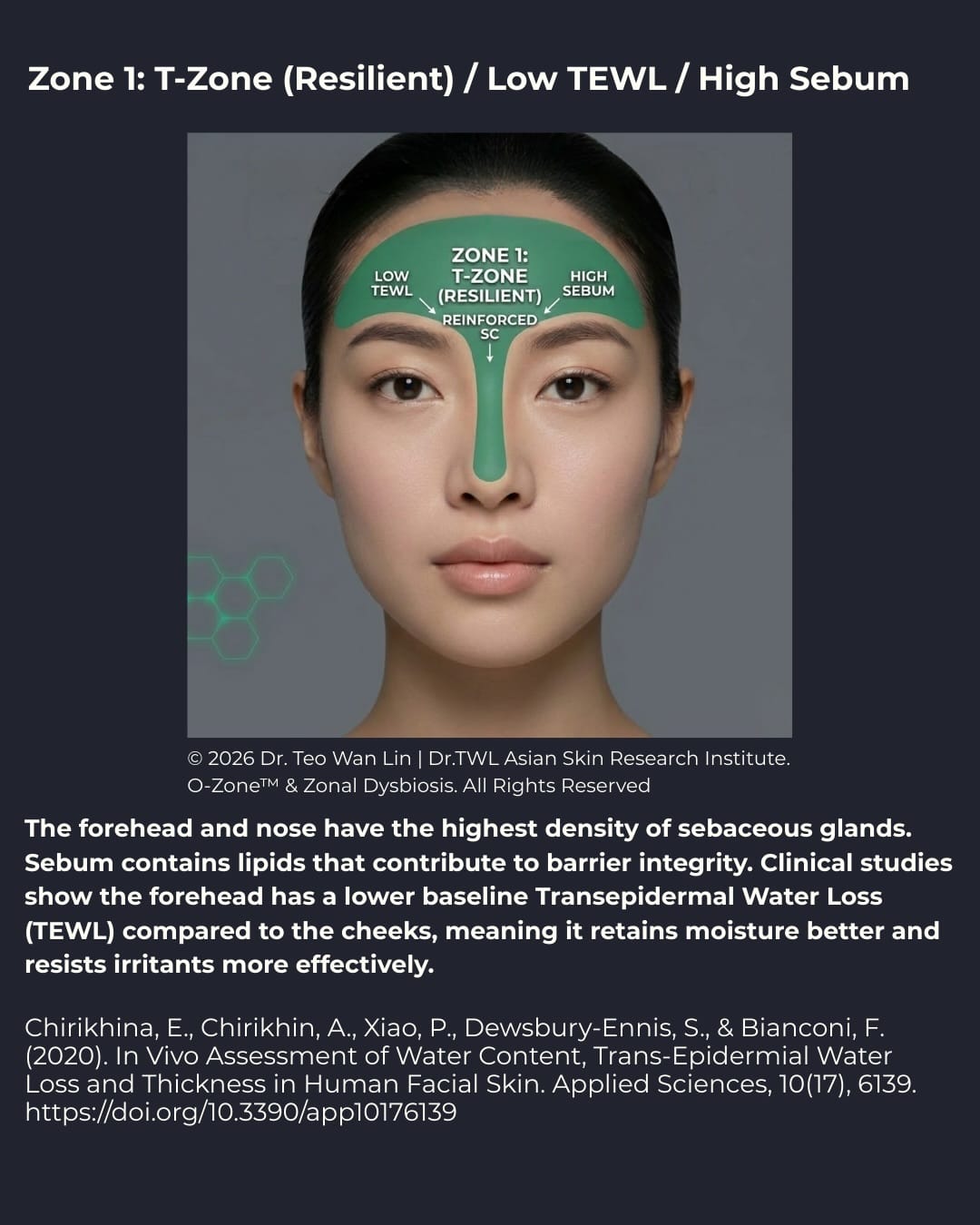
Biophysically, the skin in these areas is known to be much thinner, whereas the T-zone (forehead and nose) is generally much more resilient.
Genetic Factors in East Asians
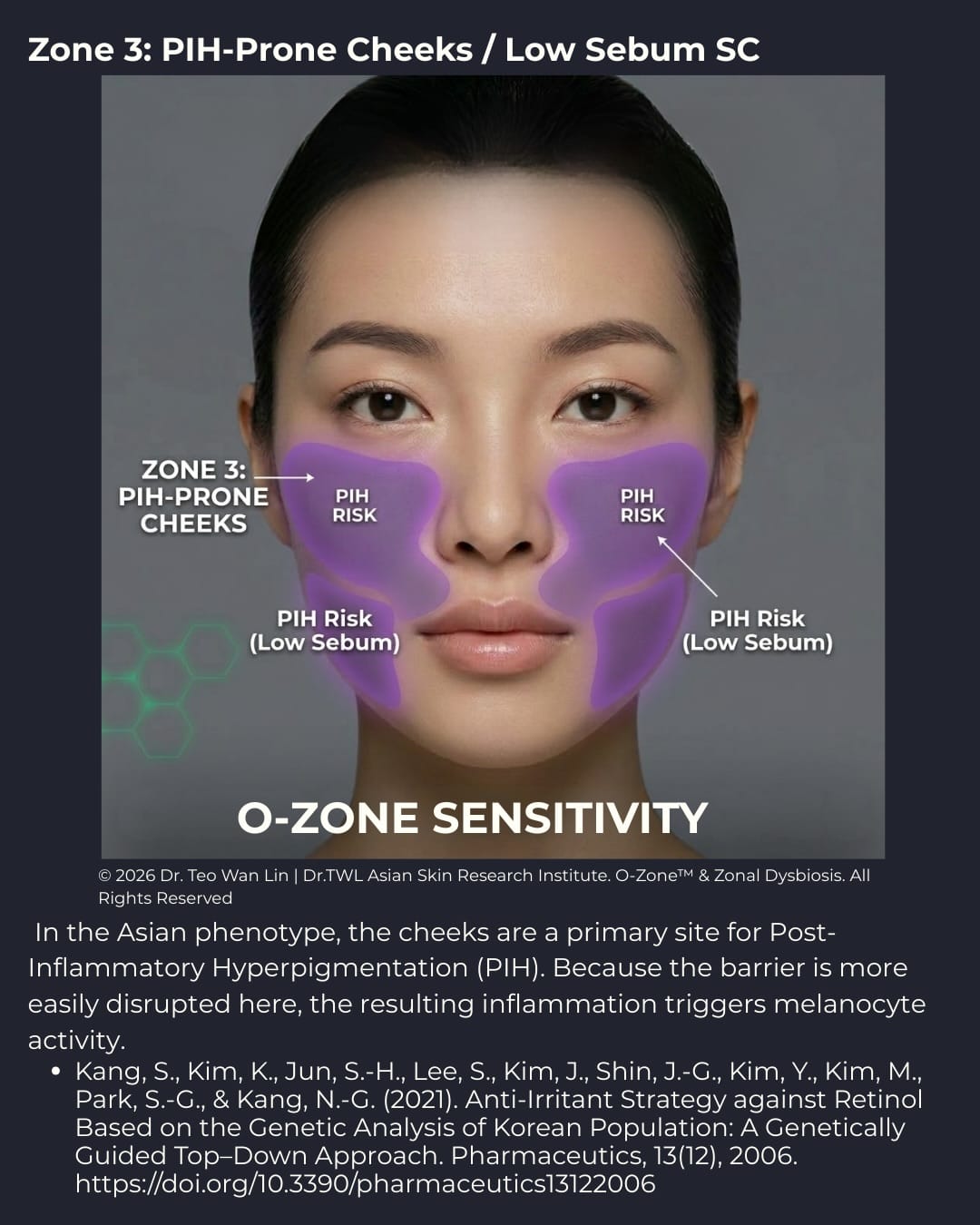
Studies prove that East Asians are genetically susceptible to retinol/retinoid sensitivity. Because East Asian skin generally has a naturally thinner stratum corneum and a higher baseline for transepidermal water loss compared to Caucasian skin, Western formulations of high-strength retinoid protocols often trigger more severe erythema and PIH (Post-Inflammatory Hyperpigmentation).
Recommendations and Alternatives
If you are experiencing skin irritation or find that retinoids no longer work for you:
- Get reviewed by a dermatologist, especially if you have active irritation.
- Understand that aging can unmask xerotic eczema, as your skin produces fewer lipids over time.
- Do not use retinoids without medical supervision if you have perioral dermatitis.
Gentler Options
There are gentler variants and esters, such as retinyl propionate. When paired with ethnobotanicals like Cica (Centella Asiatica), they can help reduce skin irritation.
Conclusion
Good skincare isn’t complicated, but biological inflammation can be confusing. While part of the efficacy of retinoids comes from stimulating dermal collagen, not all skin is the same.
The takeaway: No, retinoids do not thin the skin. Histological evidence shows they cause epidermal compaction and induce collagen formation. However, your skin changes as you age, and genetic factors play a significant role in how you tolerate them.
[Bonus Resource] The Retinoid Introduction Protocol: For Sensitive Asian Skin
Dermatologist’s Note: Retinoid therapy is a marathon, not a sprint. Because Asian skin often presents with a thinner stratum corneum and higher sensitivity (TEWL—Transepidermal Water Loss), a “Low and Slow” approach is clinically preferred.
1. The Sandwich Technique (Barrier First)
To mitigate the risk of Retinoid Dermatitis, always apply your retinoid between layers of a ceramide-dominant moisturizer.
- Step A: Apply a thin layer of ceramide-rich cream to damp skin.
- Step B: Wait 5 minutes until skin is dry to the touch.
- Step C: Apply a pea-sized amount of retinoid.
- Step D: Seal with a second layer of moisturizer.
2. The 2 X a Week Method
If you have a history of reactive/sensitive skin (not for those with eczema or other known dermatological conditions which are contraindicated for retinoid use)
- Apply your retinoid twice a week following the sandwich method with your intensive barrier repair cream.
- This allows the retinoid to signal dermal remodelling while providing barrier protection
- 3. Strategic “No-Go” Zones
Avoid applying retinoids to the following high-vulnerability areas where the stratum corneum is thinnest:
- The Periorbital Area: The corners of the eyes.
- The Nasolabial Folds: The creases around the nose.
- The Perioral Area: The corners of the mouth.
- Tip: Protect these areas with a thick occlusive (like a petrolatum-based balm) before applying your retinoid.
4. The 1-2-3 Frequency Scale
- Weeks 1–2: Apply only once a week.
- Weeks 3–4: Increase to twice a week (e.g., Monday and Thursday).
- Week 5+: Move to every other night only if there is zero redness or flaking.
5. The Red Flag Rule
If your skin feels tight, stings when applying regular moisturizer, or shows visible flaking: Stop immediately. Focus on barrier repair for 72 hours before attempting a lower frequency.
Ready to start your journey?
If you have questions about your specific skin type or concerns like eczema, always consult your dermatologist to ensure your dose and frequency are precisely controlled.
References
- Dermal Thickening: Griffiths, C. E., Russman, A. N., Majmudar, G., Singer, R. S., Hamilton, T. A., & Voorhees, J. J. (1993). Restoration of collagen formation in photodamaged human skin by tretinoin (retinoic acid). The New England Journal of Medicine, 329(8), 530–535. https://doi.org/10.1056/NEJM199308193290803
- Barrier Disruption & TEWL: Elias, P. M. (2005). Stratum corneum defensive functions: an integrated view. Journal of Investigative Dermatology, 125(2), 183-200. https://doi.org/10.1111/j.0022-202X.2005.23668.x
- Asian Skin Phenotype (TEWL Differences): Kompaore, F., Marty, J. P., & Dupont, C. (1993). In vivo evaluation of the stratum corneum barrier function in blacks, Caucasians and Asians with two noninvasive methods. Skin Pharmacology, 6(3), 200-207. https://doi.org/10.1159/000211135
- Kang, S., Kim, K., Jun, S.-H., Lee, S., Kim, J., Shin, J.-G., Kim, Y., Kim, M., Park, S.-G., & Kang, N.-G. (2021). Anti-Irritant Strategy against Retinol Based on the Genetic Analysis of Korean Population: A Genetically Guided Top–Down Approach. Pharmaceutics, 13(12), 2006. https://doi.org/10.3390/pharmaceutics13122006
- Microbiome & Retinoids:
- Xu YN, Pu M, Raut J, Du Y, Qiu Q, Hermanson K, Xu Y, Doraiswamy C, Chu CC. Skin microbiome as a signature of premature ageing: enhancement with a retinyl propionate-containing topical product. Br J Dermatol. 2025 Oct 21;193(Suppl 2):ii24-ii31. https://doi.org/10.1093/bjd/ljaf098
- Kang, S., Kim, K., Jun, S.-H., Lee, S., Kim, J., Shin, J.-G., Kim, Y., Kim, M., Park, S.-G., & Kang, N.-G. (2021). Anti-Irritant Strategy against Retinol Based on the Genetic Analysis of Korean Population: A Genetically Guided Top–Down Approach. Pharmaceutics, 13(12), 2006. https://doi.org/10.3390/pharmaceutics13122006